每个卵圆孔未闭都应该被封堵
摘要
目前,卵圆孔未闭(PFO)并未得到应有的医学重视。PFO对人类健康甚至生命构成了严重威胁。医学文献中首例相关病例报告可追溯到19世纪,其结局是死亡。约25%的人群存在PFO,这一比例突显了其潜在危害。然而,PFO的高发病率也在一定程度上使医学界对其筛查和治疗的积极性降低。约5%的人群患有高危PFO,这类PFO足以导致如死亡、卒中、心肌梗死,以及眼部、内脏和外周动脉栓塞等临床症状,因此值得进行筛查。鉴于上述重大健康风险,PFO封堵应作为一种初级预防手段。该手术也是心脏病学中最简单的干预措施之一,同时可能具有最高的临床效益。作为一种主要的预防性措施,PFO封堵可以被视为一种机械疫苗接种。在为治疗罕见适应证(如偏头痛、体位性低氧血症等)进行PFO封堵时,患者还能获得终身免疫于反常性栓塞的附加益处。反之,为预防反常性栓塞进行的PFO封堵,不仅能改善甚至治愈偏头痛或运动性呼吸困难,还能通过这些附加的益处提升患者的生活质量。
At present, the patent foramen ovale (PFO) does not receive the deserved medical attention. The PFO poses a serious threat to health and even the life of mankind. The first respective case report in the medical literature dates back to the 19th century. It led to death. The fact that a PFO is present in roughly 25% of people underscores its overall potential to cause harm. Yet at the same time, the sheer number discourages the medical community from screening for it and from treating it. About 5% of the population have particularly dangerous forms of PFOs. Such PFOs portray a high enough risk for clinical events, the likes of death, stroke, myocardial infarction, or ocular, visceral, and peripheral embolism, to justify screening for them. Highly significant health incidents being at stake, it appears obvious that PFO closure should be used for primary prevention. This is supported by the fact that closing a PFO is the simplest intervention in cardiology, with presumably the highest clinical yield. Being mainly a preventive measure, PFO closure represents a mechanical vaccination. When closing PFOs for one of the rarer therapeutic indications (migraine, platypnea orthodeoxia, etc.), patients automatically profit from the collateral benefit of getting, at the same time, mechanically vaccinated for life against paradoxical embolism. Vice versa, closing a PFO for the prevention of paradoxical embolism betters or cures migraine or exercise dyspnea not infrequently, thereby improving quality of life as a collateral benefit.
关键词:心绞痛;房间隔缺损;附加益处;封堵器封堵;左心耳;机械疫苗接种;偏头痛;心肌梗死;卵圆孔未闭;反常性栓塞;外周栓塞;初级预防;卒中;短暂性脑缺血发作;
PART/1
引言
利用经皮PFO封堵器进行PFO封堵已有30多年的历史[1]。第一款专门针对PFO设计的——Amplatzer PFO封堵器,于1997年9月10日首次使用[2]。作为在当时介入心脏病学中唯一的产品,自首次用于人体以来,该产品并未经历重大改进,也无需如此。截至目前,Amplatzer PFO封堵器已在数十万甚至数百万患者中几乎完美地发挥了作用。毫不奇怪,它已衍生出相当数量的仿制品和衍生产品。
The closure of a patent foramen ovale (PFO) with a percutaneous occluder device has been around for over 30 years [1]. A dedicated device for the PFO, the Amplatzer PFO Occluder, was first used on 10 September 1997[2]. As practically the only device in interventional cardiology, it has not needed, and therefore not seen, any significant iteration since its first-in-man use. To date, the Amplatzer PFO Occluder has gathered an impressive record to have worked virtually flawlessly in hundreds of thousands, if not millions, of patients. It comes as no surprise that the device has begot a fair number of duplicates and derivatives.
PART/2
PFO封堵手术
使用Amplatzer封堵器或类似产品进行PFO封堵的手术极其简单、无害且有效。经过一段短暂而快速的学习过程后,任何介入心脏病学医生都可以在不到30分钟内完成此操作。无需对患者进行镇静处理。实际上,患者完全可以在离开导管室时像献血后握住肘部一样握住股静脉穿刺部位。术后对患者的身体活动没有限制,患者可以在同一天进行包括水下潜水在内等运动。
Closing a PFO with an Amplatzer occluder or a comparable device is extremely simple, innocuous, and effective. After a short and steep learning curve, it can be accomplished by any invasive cardiologist within less than 30 min. There is no necessity for sedation of patients. In fact, there is no reason for them not to leave the catheterization laboratory on foot holding the venous femoral puncture like one holds the elbow after donating blood.
术后药物治疗可以简化为每日100毫克阿司匹林,持续一个月或两个月,无需预加载或负荷剂量。基本不会出现术后问题,因而不需要进一步的医学随访。然而,为了排除临床上显著的残余分流风险(预计发生率低于10%),建议在术后3至6个月进行持续Valsalva动作后的经胸超声心动图(TTE)和发泡试验。需要对比经食管超声心动图(TEE)检查以发现小的残余分流(约20%的病例中可观察到,但在大多数情况下临床上无关紧要)或明显的附着血栓(发生率不到1/500)。大多数医生和患者希望确保手术万无一失,因此在大多数医疗机构中,术后TTE或TEE对比检查已成为标准流程。
There are no physical restrictions after such a PFO closure and even sports including underwater diving are possible on the same day. Medical treatment after the procedure can be stripped down to 100 mg of acetylsalicylic acid daily for a month or two without a preloading or loading dose. Later problems to be looked for are so rare that no further checkups are medically required. Nonetheless, for ruling out a clinically significant residual shunt (to be expected in less than 10% of cases), it is recommendable to perform a transthoracic contrast echocardiogram (TTE) with a bubble test at the end of a sustained Valsalva maneuver after 3 to 6 months. To also reliably uncover small residual shunts (to be expected in about 20% of cases, but clinically irrelevant in most instances) or significant thrombi on the device (a risk of less than 1 in 500), a contrast transesophageal echocardiogram (TEE) is required. Most physicians and patients want to make sure that everything is perfect, and follow-up contrast TTEs or TEEs are standard in the majority of institutions.
这是一种当天即可完成的经济方便的手术,仅依靠透视引导即可完成。患者通常带着静脉输液管来到导管室,已提前接受一些静脉注射或口服抗生素以预防感染。手术从右侧腹股沟的局部麻醉、经皮小切口以及静脉注射5000单位的肝素开始。
The intervention in its economical and frugal version is a same-day procedure, guided solely by fluoroscopy. The patient usually arrives at the catheterization laboratory with a venous line, having received some prophylactic intravenous or oral antibiotics. The intervention starts with a local anesthesia at the right groin, a small skin incision, and an intravenous bolus of 5000 units of heparin.
通过穿刺针穿刺股静脉后,插入一根带有U形头的常规0.035英寸导丝。在接近一半的病例中,导丝从下腔静脉通过右心房向上推进时,会自然穿过PFO进入左心房。如果导丝未能一次通过,可以在右心房内多次重新尝试,因为导丝可能不会在第一次就通过,但在接下来的尝试中成功的概率会增加。使用带有U形头的导丝首次尝试穿过房间隔时,利用的是其只能通过裂隙状PFO的特性。而直导丝或导管可能会意外穿过原发隔中的微小房间隔缺损(ASD)。小的筛孔状ASD在术前的超声心动图检查中通常会被忽略。
The femoral vein is punctured, and a conventional 0.035’’ guidewire with a U-tip is through the puncture needle. In nearly half of cases, the guidewire spontaneously passes the PFO into the left atrium when advanced up from the inferior vena cava through the right atrium. If not, it pays out to recross the right atrium a couple of times, because the wire may not pass at first but rather at one of the following attempts. The initial attempt to pass the atrial septum with a U-tip wire tries to take advantage of the fact that the U-tip wire can only pass through the slit-like PFO. A straight wire or a catheter may inadvertently pass through a tiny atrial septal defect (ASD) in the septum primum. Small cribriform ASDs often go unnoticed in prior echocardiograms.
如果导丝未能通过,可在无需鞘管的情况下在导丝上插入一根4F到6F的多功能导管。为了使导管能够进入静脉,可能需要旋转导管穿过皮肤和紧张的皮下组织。多功能导管随后停放在膈肌水平,指向左肩(即正面视图的2点钟方向)。此时,将导丝多次深入右心房,直到导丝到达2点钟位置。这通常意味着导丝已经进入左心房。在正面视图中,如果导丝意外经过右心室进入左肺动脉,可能会出现类似的导丝轨迹。然而,在导丝推进过程中,几乎总会伴随室性异位心搏。通过左前斜位或侧位检查导丝位置,可辨别导丝是否错误地经过右心室进入肺动脉。如果导丝在屏幕左侧靠近胸骨处形成弓状,则说明导丝误入右心室后进入肺动脉。相反,如果导丝在该视图中在屏幕右侧呈直线,则表明导丝已正确通过PFO进入左心房。
If the wire fails to pass, a 4 to 6 French (F) multipurpose catheter is inserted over the wire without a sheath. It may be necessary to actually screw the catheter through the skin and any tense subcutaneous tissue to be able to enter the vein over a regular guidewire. The multipurpose catheter is then parked at the level of the diaphragm pointing to the left shoulder, i.e., to 2 o’clock, in a frontal view. The wire is advanced several times deep into the right atrium until it arrives at the 2 o’clock position. This usually means that the left atrium is reached. In the frontal view, a similar wire trace may appear with an inadvertent route through the right ventricle into the left pulmonary artery. This path, however, almost invariably causes ventricular ectopy during wire advancement. After checking the wire position in a left anterior oblique or lateral view, the erroneous passage through the right ventricle into a pulmonary artery is identified by a bow of the wire on the left side of the screen close to the sternum. The correct route into the left atrium through the PFO shows the wire straight on the right side of the screen in that view.
如果改变多功能导管的方向和位置后仍然无法通过PFO,可以取出U型导丝,并用拇指指甲刮直导丝的弯曲部分。如果刮直后的导丝仍无法通过,可用多功能导管的尖端继续寻找PFO的入口。如果以上方法均失败,则需通过注射造影剂进行右心房造影以了解解剖结构(如图1所示)。
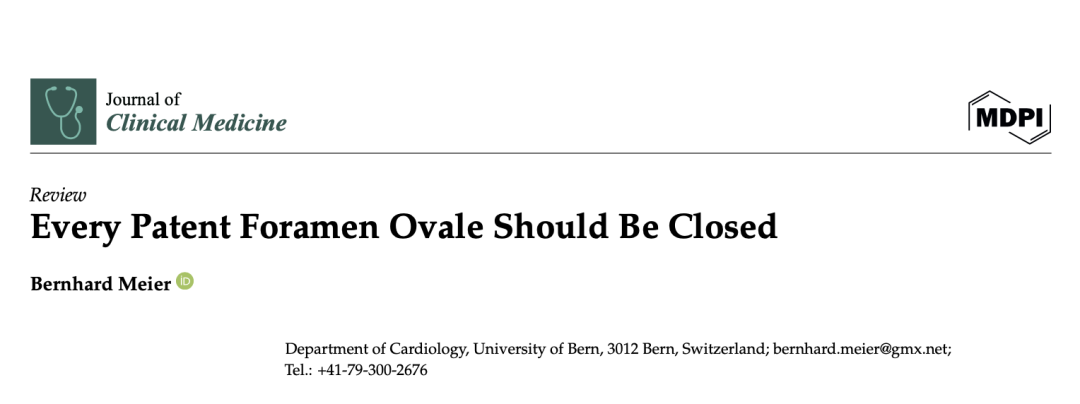
If the PFO cannot be passed despite changing the direction and position of the multipurpose catheter, the U-tip wire may be removed and the tip straightened by scratching the back of the curve with the thumb nail. Should the now straight wire still not pass, the PFO is searched for with the tip of the multipurpose catheter. If even that fails, a right atriogram with contrast medium is performed to understand the anatomy (Figure 1).
一旦成功穿过PFO,导丝需保留在其原始到达的位置,无论是左心房本身、左心耳(LAA)还是肺静脉。如果使用了多功能导管,此时需将其移除。对于身材高大的患者,标准长度的导丝可能太短,无法在移除多功能导管时手动保持导丝尖端在左心房内。这种情况下,可以在导丝的远端尖端进入导管近端后,连接一个小口径注射器或动力注射器,通过多功能导管强力注射生理盐水或造影剂,同时完全撤出多功能导管,从而使导丝保持在左心房内。特别是在由第二人注射或使用动力注射器的情况下,当多功能导管尖端即将撤出时,操作人员需手动防止其移动,以避免导管失控弹出,并伴随注射液飞溅至周围环境。
Once the PFO is crossed, the guidewire is kept wherever it spontaneously wound up, be that the left atrium itself, the left atrial appendage (LAA), or a pulmonary vein. In the cases it was used, the multipurpose catheter is now removed. In tall patients, a regular-length guidewire may be too short to manually keep the guidewire tip in the left atrium while exiting the multipurpose catheter. A small caliber syringe or a power injector can be connected to the multipurpose catheter once the distal tip of the wire has vanished into the proximal end of the catheter to forcefully inject saline or contrast medium while the multipurpose catheter is fully withdrawn. This keeps the wire still in the left atrium. Particularly if a second person injects or a power injector is used, the tip of the multipurpose catheter has to be manually stopped by the operator as soon as it exits the skin to avoid uncontrolled ejection of the catheter accompanied by a shower to the environment with the injected fluid.
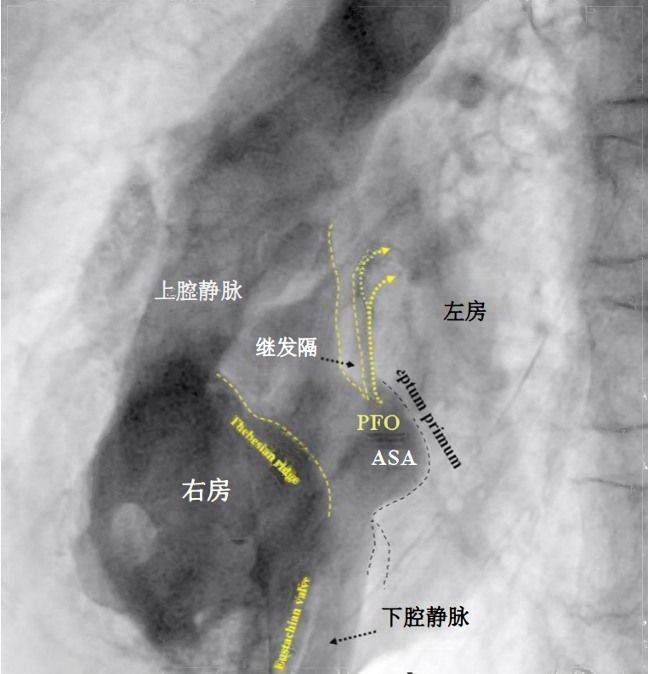
图1.PFO的透视对比成像(左前斜位视图)
所有重要特征均清晰可见,包括欧氏瓣和冠状窦瓣(右心房游离壁上的一个突起,可与房间隔混淆)ASA = 房间隔瘤(atrial septal aneurysm)
一旦移除多功能导管,需要检查穿刺点是否只有静脉出血。如果发现动脉出血,则需要重新穿刺。这种情况表明股静脉可能被误穿过动脉后进入。必须避免将用于输送封堵器的8到10F鞘管通过动脉内导丝插入股静脉,该导丝若通过动脉进入股静脉会带来风险。在上述常见情况下,导丝可能直接穿过PFO,而未使用多功能导管。在完全插入输送鞘之前,同样重要的是检查是否准确地进入股静脉。这可以通过先前推鞘管的锥形尖端,然后短暂撤回以确认仅有静脉出血来实现。
As soon as the multipurpose catheter is removed, the puncture site is inspected for exclusively venous bleeding. If there is arterial bleeding, a new puncture will be required. It has to be assumed that the femoral vein was inadvertently entered by traversing an artery. For obvious reasons, it must be avoided to insert the 8 to 10 F sheath required for device delivery over a wire passing through an artery into the femoral vein. In the mentioned frequent cases, the wire had passed directly through the PFO without using a multipurpose catheter; it is equally important to check the access path into the femoral vein before fully inserting the delivery sheath. This is achieved by advancing only the tapered tip of the sheath and then withdrawing it briefly to ascertain venous-only bleeding.
输送鞘可以直接穿过导丝,为了避免导丝弯曲,建议通过旋转动作使鞘管穿过皮肤进入股静脉。一旦进入后,路径就会变得笔直,不再需要额外的导丝刚性来克服阻力。
The sheath required for device implantation can be inserted over the regular guidewire in place. For passing through the skin into the femoral vein, a screwing rotation is recommended to avoid wire kinking. After that, the path is straight and no more resistance will occur that would require additional stiffness of the guidewire.
进入左心房后,移除鞘管的扩张鞘(厚壁内件),并通过将鞘管外端保持在或低于患者心房水平来确认左心房动脉血的反流。这是整个操作过程中鞘管应保持的位置。
Once in the left atrium,the obturator (thick-wall inner part) of the sheath is removed and backflow of arterial blood from the left atrium is ascertained, with the outer end of the sheath held at or below atrial level at the side of the patient. This is where the sheath should be kept and handled throughout the entire case.
将选好的封堵器收纳至冲洗过后的装载器,并确保封堵器的尖端微微露出,然后将其与输送鞘连接。在不进行任何冲洗的同时,将封堵器输送至鞘管头端。在推出封堵器之前,确保Amplatzer封堵器及其大多数衍生产品的铆头适当拧紧,但不要过紧。铆头和钢缆之间应有一个小间隙(如图2所示)。如果没有间隙,建议逆时针旋转螺钉一到两圈,通常可以感到一个解锁的“咔嗒”声。这确保了在最终释放封堵器时,铆头不会过快拧紧而导致封堵器随着钢缆旋转而无法释放。如果间隙过大,可能使封堵器在通过鞘管时部分意外松脱。这需要通过顺时针旋转钢缆来纠正。在极其罕见的情况下,如果发现铆头完全断开,则不应植入封堵器,而是用圈套器从鞘管中捞出封堵器,重新正确连接后再重新植入。
The flushed short loader sheath containing the selected preloaded occluder with its tip just peeking out is connected to the backbleeding sheath and the device is advanced to the distal tip of the sheath without any simultaneous flushing. Before exiting the sheath, it is made sure that the screw used for fixing the original Amplatzer device and most of its derivatives during delivery is still properly tightened, but not too much. A small gap ought to be visible (Figure 2). If there is no gap, one or two full left (counterclockwise) turns are recommended, during which an unblocking click is usually felt. This assures that the screw is not tightened overly fast so that the occluder would swivel with the loader cable rather than being released when the unscrewing is attempted at the end of occluder positioning. Too generous a gap results from inadvertent partial unscrewing of the occluder on the way up through the sheath. That needs to be corrected with turning right (clockwise) on the loading cable. In the extremely rare case that the screw is seen to be completely disconnected, the device is not implanted but pulled out of the sheath with a snare and reattached properly before reinsertion and implantation.
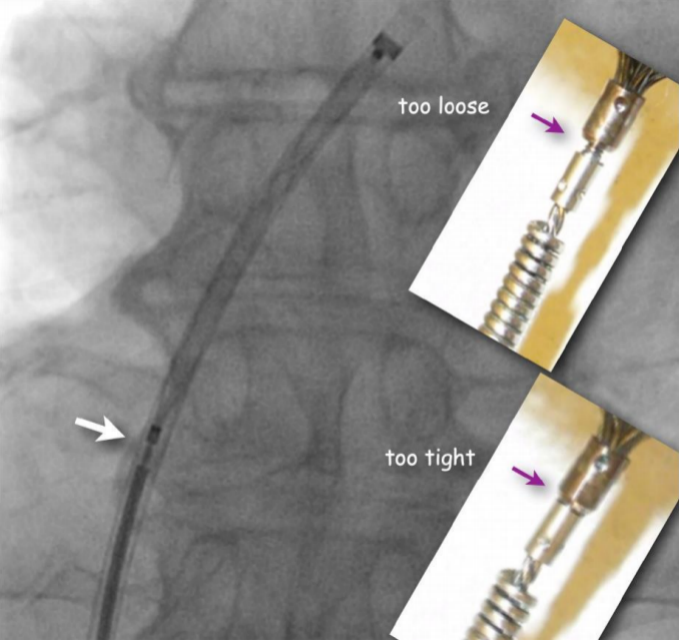
图2. 正面透视检查Amplatzer(或类似)封堵器的正确连接。
钢缆螺钉套圈与封堵器螺母之间的小间隙(白色箭头)保证封堵器安全连接,同时在定位后易于释放。插图显示了需要调整的螺钉位置,可在将封堵器推进鞘管外之前,通过顺时针(如果过松)或逆时针(如果过紧)旋转推送缆线进行校正。
剩余步骤在左前斜位透视投影下进行。将封堵器的左侧伞盘推出鞘管。最初可能看不清楚,但此时可以在鞘管尖端处看到封堵器的腰部。接着,将输送系统作为一个整体向后拉。当左侧伞盘与房间隔对齐时,其轮廓将清晰可见,特别是在左前斜位中。接下来,通过保持左盘紧贴房间隔,并继续撤回鞘管直到接近铆头的位置,释放右盘。这时,所有输送系统都应处于放松状态(不再对鞘管或装置施加拉力),右盘会自动与房间隔右侧对齐,或通过轻推使其就位。
The remaining steps are carried out in a left anterior oblique fluoroscopic projection. The left disc is pushed out of the sheath. It may not be clearly visible at first, but the waist of the device is now shown at the tip of the sheath. The system is then pulled back as a unit. As soon as the left disc aligns with the atrial septum, it will infallibly become visible in its profile in the left anterior oblique projection. Now, the right disc is released by keeping the left disc snugly cuddled to the septum and by withdrawing the sheath until proximal to the screw. At this moment, everything is relaxed (no more pulling on sheath or device) and the right disc will automatically align to the right side of the septum or it can be pushed there.
在冲洗鞘管并调整投影角度后,使两个伞盘的轮廓完全显现且无重叠的情况下,进行造影剂注射。此时可以观察到所有必要的细节(如图3所示)。然后释放封堵器,即通过旋松钢缆或使用其他封堵器的释放机制完成装置的解锁和释放。如果在释放装置时封堵器显著移动,则需要再次调整透视并进行进一步的造影剂注射。这种情况通常发生在存在房间隔瘤(ASA)或由于释放前鞘管或钢缆造成的显著位移时(如图3所示)。
A contrast medium injection is carried out after flushing the sheath and after adjusting the projection so that both discs are seen in perfect profile without any overlap. It will show all necessary details (Figure 3). The device is then released, i.e., unscrewed from the pusher cable or liberated by whatever attachment and release mechanism is used with alternative occluders. A further contrast medium injection after readjusting the projection is required only if the device moves significantly upon release. This typically happens in the presence of an atrial septal aneurysm (ASA) or due to significant position distortion by the sheath or pusher gear before release (Figure 3).
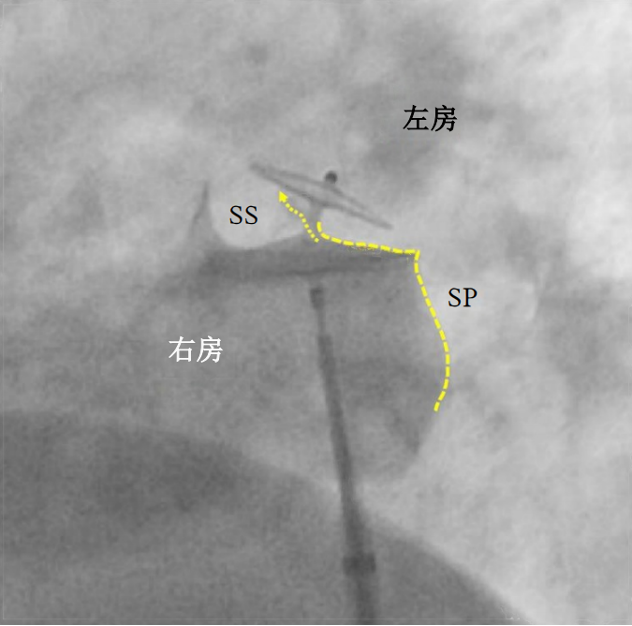
图3. PFO封堵器释放前的造影剂注射(左前斜位视图)。
25/18 mm Amplatzer PFO封堵器的左侧(头侧)部分正确贴合于继发隔(SS),称为阳性“吃豆人”征,这是安全释放的必要条件。原PFO通道现已被封堵(虚线箭头)。原发隔(SP)用虚线表示,其位于封堵器尾侧的部分是将来可能需要透视引导下经房间隔穿刺的理想位置。在类似的预释放状态下,封堵器通常在释放时会顺时针旋转约四分之一圈。最终封堵器的位置预计将更加垂直,与房间隔平行,且原发隔(SP)上不再出现压痕。
患者在鞘管移除前或移除后,可在协助下将手指放置在正确位置,舒适且安全地按压腹股沟部位。平卧时,仅需很小的压力即可,通过抵消小于10 mmHg的静脉压力来防止出血。在如此低的压力下,几乎不会形成血肿。一些医生会使用“8字缝合”关闭皮肤切口。一旦缝线或手指封堵了唯一可能的血液出口(即皮肤切口),股静脉将不再有出血的风险。然而,当患者站立时,静脉压力会突然升高,相当于从腹股沟到头顶的血柱重量,约为60 mmHg。这种情况下,需要更强的手动压迫(刚刚应用的8字缝合已不足以抵挡压力),同时还增加了血肿或通过未缝合的皮肤切口而大量出血的风险。
The patients can comfortably and safely hold the groin after having been helped to place their fingers in the right position before or after withdrawing the sheath. In a supine position, very little pressure is required to prevent bleeding by withholding venous pressure of less than 10 mmHg. A hematoma cannot form with such a low pressure. Some operators close the skin nick with a figure-of-eight suture. Once stitches or a finger block the only possible blood exit, the one through the skin, the femoral vein can no longer shed blood. When standing up, the venous pressure abruptly increases to the weight of the column of blood extending from the groin to the tip of the head. This corresponds to about 60 mmHg, requires a more robust manual compression (a just-applied figure-of-eight suture is no longer sufficient), and also carries the risk of a hematoma or copious bleeding to the outside through an unstitched skin nick.
关于封堵器的大小,使用Amplatzer封堵器时,几乎所有的PFO都可以适配两种规格:25 mm PFO封堵器(右盘25 mm,左盘18 mm)或35 mm PFO封堵器(右盘35 mm,左盘25 mm)(如图4所示)。约25%的病例需要使用35 mm封堵器,这通常包括以下情况:原发隔脆弱且活动度较大(通常称为房间隔瘤,ASA)、继发隔肥厚,或两者兼有。生产和使用左盘小于右盘的封堵器是合理的。即使使用较小的左盘,瓣叶状的PFO也能被封堵。左侧较小的伞盘可以使其减少与搏动的主动脉的接触面积,避免极少数出现但严重的PFO封堵器磨损心房的情况。右盘必须足够大,以避免封堵器从继发隔脱离(即所谓的“Pacman位置脱扣”)。这种脱离是由于右盘过小而引起的,尤其在存在ASA、继发隔肥厚或两者兼有的情况下[3]。
Regarding occluder size, practically all PFOs can be fit with either a 25 mm PFO occluder (right disc 25 mm and left disc 18 mm) or a 35 mm PFO occluder (35 mm, 25 mm), when using Amplatzer occluders (Figure 4). The 35 mm occluder will be required in about 25% of cases, those with either a marked frailty and mobility of the septum primum (generally referred to as ASA), a lipomatous (thick triangular) septum secundum, or both. The production and use of occluders with a smaller left disc than the right disc make sense. The flap-valve-like PFO will be pulled shut even by a small left disc. A smaller disc on the left side reduces overall contact with the pulsating aorta, the most common cause of the rare but ominous erosion of a free atrial wall by a PFO occluder. The right disc must be large enough to avoid disengagement from the septum secundum. This problem is also called unhinging from the Pacman position and is the consequence of too small a right disc in the presence of an ASA, a lipomatous septum secundum, or both [3].

图4.PFO封堵器尺寸选择简化示意图。
隧道长度不重要。ASA = 房间隔瘤;SP = 原发隔;SS = 继发隔。
PART/3
何时及如何筛查PFO
静脉血栓栓塞症,是PFO造成伤害的先决条件,在青春期晚期之前几乎不是问题,其发病率会随着年龄增长和合并疾病的增加而呈指数增长[4,5]。口服避孕药可能在存在PFO的情况下增加早期反常性栓塞的风险。年轻人中偏头痛是PFO筛查的重要指征。PFO封堵治疗偏头痛不仅有较大的缓解症状的机会[6],还提供了一个附带的终身初级预防益处——反常性栓塞的“机械疫苗”[7]。
Venous thromboembolism, the prerequisite for a PFO to cause harm, is hardly an issue until late adolescence but its incidence exponentially increases with older age [4,5] and with morbidity. Oral contraception represents an early potential harbinger of paradoxical embolism in the presence of a PFO. Migraine in young people constitutes an attractive indication for PFO screening. PFO closure for migraine has a good chance for symptomatic relief [6] and offers, as a collateral bonus, lifelong primary prevention—mechanical vaccination[7]—against later paradoxical embolism.
筛查危险的PFO(如较大的PFO或合并房间隔瘤(ASA)[8]、欧氏瓣[9-12]或希阿里氏网[13]相关的PFO),经胸对比超声心动图(TTE)发泡试验即可满足需求(图5)。造影剂需要在持续Valsalva动作结束时注射。做Valsalva动作或由医护人员在经食管超声心动图(TEE)期间由按压患者上腹部,可阻止静脉血回流到胸腔。此时,双心房的容量在10至20秒内显著减少。Valsalva动作或按压结束时,静脉血迅速涌入右心房,从而推动PFO向尚未充盈的左心房打开。
To screen for dangerous PFOs, i.e., large ones or those associated with an ASA [8], a Eustachian valve [9–12], or a Chiari network [13], a bubble test during a TTE suffices (Figure 5). The contrast liquid has to be injected at the end of a sustained Valsalva maneuver. A Valsalva maneuver, or pressing into the upper belly by a medical person during TEE if a sedated patient cannot perform a Valsalva maneuver, blocks the backflow of the venous blood into the thorax. Both atria become volume-depleted within 10 to 20 s. Upon Valsalva or pressing release, the venous blood gushes into the right atrium first, thereby pushing the PFO open towards the still underfilled left atrium.
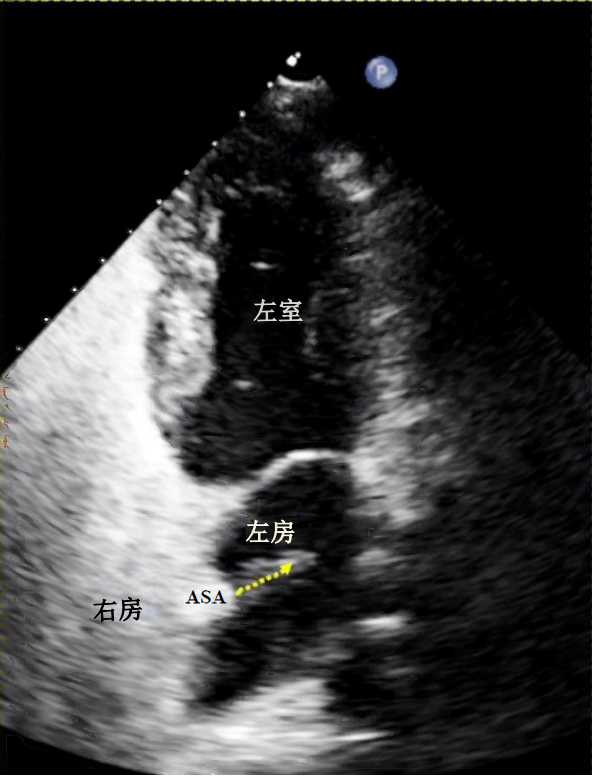
图5. 经胸超声心动图证实PFO伴右向左分流。显示了一个起源于房间隔瘤(ASA)区域的右向左气泡分流(虚线箭头)。
下腔静脉流入右心房的静脉血流直接指向PFO,尤其是在存在欧氏瓣[9-12]或希阿里氏网[13]的情况下。相比之下,上腔静脉的血流并不会直接指向PFO。因此,理想情况下,造影剂应注射到腿部静脉[14,15]。然而,这在实际操作中不太方便,大多数情况下需选择手臂静脉注射。在经食管超声心动图(TEE)或经颅多普勒检查(TCD)中进行的发泡试验,还可以检测到较小的PFO,尽管这些PFO风险较低,但仍可能导致反常性栓塞的相关风险[16]。
The venous inflow into the right atrium from the inferior vena cava is directed onto the PFO, even more so in the presence of a Eustachian valve [9–12] or a Chiari network [13]. The inflow of the superior vena cava is not. Hence, injecting the contrast medium in a leg vein would be ideal [14,15]. Yet this is impractical, and under most circumstances, an arm vein has to do. A state-of-the-art bubble test during a TEE or a transcranial Doppler examination [16] in addition detects small PFOs that harbour a smaller (albeit still relevant) risk for paradoxical embolism.
耳血氧仪是20多年前首次发表的一种有趣的PFO筛查技术[17]。然而遗憾的是,自2013年以来,这一技术没有再得到进一步的探讨[18]。耳血氧仪是唯一一个可以应用于学校教室和商场的检测方式。先证者让受试者持续执行Valsalva动作,并将图解血氧计连接在患者耳垂上。在处于Valsalva动作的呼气状态时,若有任何大孔的PFO短暂开放,静脉血会有一过性血流通过PFO并到达耳垂。血氧饱和度曲线将瞬间下降。倾斜的深度和宽度对应了PFO的严重性[18]。
Ear oximetry represents an interesting PFO screening technique first published over 20 years ago [17]. Regrettably, it has not been further pursued since 2013 [18]. It is the only screening method that could be applied in school classrooms or shopping malls. The proband performs a sustained Valsalva maneuver with a graphical oximeter attached to an ear lobe. At the Valsalva release, when any large PFO will briefly open, a small tsunami of venous blood will run through the PFO to reach the ear lobe. The oxygen saturation curve dips momentarily. The depth and width of the dip correspond to the importance of the PFO[18].
很显然,即便是这样一个简单的测试,想要筛查整个世界的人口,医疗后勤和资金仍然是缺乏的。话虽如此,所有情况下,哪怕只是稍微有一点点PFO可能性,都应该被认为是进行筛选测试的理由和机会。例如在与偏头痛相关的神经学领域症状,尤其但不特指先兆性偏头痛,以及任何大脑疾病相关的问题(不仅仅是年轻和其他健康患者的所谓的不明原因事件)。PFO在老年人和病弱者中更容易引起反常性栓塞,因为他们更容易发生静脉血栓栓塞,这是反常性栓塞的前提条件。PFO携带者的绝对风险随年龄和疾病呈几何级数增加。由于累积性原因导致全身性动脉闭塞,带来了综合危害,从而导致PFO的相对风险下降。在心血管领域,如果患者监测出有PFO并伴有血管栓塞导致的心肌梗死,那么需要进行封堵。拥有伴随性粥样硬化也同样需要封堵PFO,否则会增加心肌梗死的风险。动脉粥样硬化和静脉血栓的患病率随着年龄和合并症的增加而增加。心血管学家应该多质疑——基于血管在系统性循环中的分布,因为神经科医生确诊的每3例PFO相关脑疾病中就有一个PFO相关性心梗。另外要补充的一点是,PFO相关性脑疾病很大程度被漏诊,因为诊断人群仍然局限在年轻人和其他健康人群,而这些人很明显是拥有个体风险最小的人群。
Obviously, even with such a simple test, medical logistics and funding are lacking to screen the world population. Having said that, every situation even remotely reminiscent of a PFO problem should be considered a reason and opportunity for a screening test. In the realm of neurology that pertains to migraine, particularly but not exclusively if associated with aura, and to any cerebral event (not only to those called cryptogenic in young and otherwise healthy patients). The PFO causes more paradoxical embolism in old and sick people because of their propensity for venous thromboembolism, the prerequisite for paradoxical embolism. The absolute respective risk for PFO carriers increases geometrically with age and disease. The relative risk decreases due to the aggregated hazard of accumulating competitive causes for systemic arterial occlusions. In the realm of cardiology, one should screen for a PFO and occlude it if found with every myocardial infarction (MI) that looks in any way embolic. Concomitant atherosclerosis by no means acquits the PFO. It rather heightens its risk to cause an MI. The prevalence of both atherosclerosis and venous thrombosis grows in unison with age and comorbidities. Cardiologists should suspect—based on the blood volume distribution in the systemic circulation—one PFO-associated MI per every three PFO-associated cerebral events identified by neurologists. We can add to this that PFO-associated cerebral events are grossly underdiagnosed as they are still only looked for in young and otherwise fit patients, notably the patient group with the lowest absolute respective risk.
忽视PFO的筛查只是导致PFO封堵术使用不足的原因之一,另一个原因是,人们错误地认为,最初与PFO相关的事件是良性的,因此没有及时闭合。历史上发生的第一例PFO事件就是致命的[19]。拥有PFO的患者人口数量随着年龄的增长而降低[20,21],这表明PFO患者存在选择性死亡。此外,在PFO和指示症状患者的倾向匹配比较中,大约150名接受PFO封堵术的受试者在10年随访期间的死亡率明显低于纯药物治疗的相同数量的受试者[22]。
Neglected screening for a PFO is only one of the reasons for underused closure of PFOs. Another reason is the false assumption that first PFO-related events be benign and leave time for reaction. PFO case number one in the medical literature was fatal [19]. PFO carriers as a percentage of the population decrease with age [20,21], pointing to selective mortality of people with a PFO. Moreover, in a propensity-matched comparison among patients with a PFO and an index event, mortality was significantly lower over ten years of follow-up in the about 150 subjects with PFO closure than in the same number with purely medical treatment [22].
PFO万分需要引起应有的关注。PFO封堵能够有效地解决潜在的危及生命的问题,其干预措施的复杂性与修复牙齿相当。术后仅仅几个小时,患者的生活就能完全恢复正常。临床操作技术的成功率几乎为100%。长期临床有效性超过90%。巨大的长期问题几乎没有。PFO封堵的费用实际开销少于10000欧元。
PFOs direly need to receive the medical attention they deserve. PFO closure effectively addresses potentially life-threatening problems with an intervention comparable, in intricacy, to mending teeth. Completely normal life resumes as soon as a couple of hours after the act. The technical success rate is virtually 100%. The long-term clinical efficacy is over 90%. Significant late problems are exotically rare. Actual costs of PFO closure amount to less than EUR 10,000.
无论是否已知脑事件发生的原因,如动脉粥样硬化或心房颤动(AF),都必须寻找PFO。它是此类事故的潜在罪魁祸首,也是最容易诊断和消除的。有趣的是,隐源性卒中一词最初包含房颤的患者。然而在这之后,房颤成为脑卒中的一种已发现的病因。这是有道理的,但将PFO列为非隐源性脑卒中发生原因,并把它移出未确定来源的栓塞性卒中组列(ESUS),同样是有理,甚至是非常正确的[23]。表格1列出了栓塞事件的分类。与高风险的PFO相比,发作性房颤引起栓塞事件的可能性要小得多,发作时间短且罕见。无论是在PFO还是房颤导致的卒中,卒中的发生原因常常只是被假定,而没有被确诊,罕见例子除外[24,25]。关于房颤需要终身口服抗凝药物,同时也可以预防PFO介导的事件,可以从两个方面被反驳。首先,由于患者依从性差和必要时需要暂停的特点,口服抗凝药只提供有限的防护。PFO和左心耳(LAA)封堵术易于联合进行(仅增加几分钟手术时间和第二个封堵器的费用)[26],从而避免了因心房颤动而持续增加的出血风险(该风险随年龄增长呈指数级上升),也避免了服用口服抗凝药的需要。机械性预防一词适用于PFO[7]和LAA[27]封堵术,两者都不存在依从性问题。
Irrespective of the presence of established causes of cerebral events, such as atherosclerosis or atrial fibrillation (AF), the PFO must be looked for. It is a potential culprit for any such accident—the easiest to diagnose and to eliminate, for that matter. Interestingly, the term cryptogenic strokes initially encompassed patients with AF. Only later, AF was promoted to an established cause of stroke. That made sense, but it makes equal sense and is overdue to classify a PFO as a non-cryptogenic stroke cause and also remove it from the basket of embolic stroke of undetermined source called ESUS [23]. Table 1 proposes an adapted classification of embolic events. The potential to cause an embolic event of paroxysmal AF with rare and short episodes is much smaller than that of a high-risk PFO. In both cases, the stroke cause is usually assumed and not proved, with rare exceptions [24,25]. The argument that AF requires oral anticoagulation (OAC) for life, which, at the same time, protects against PFO-mediated events, can be rebutted in two ways. First, OAC provides only limited protection due to its notoriously poor compliance and required pauses. Second, easily combinable PFO and LAA closure (adding only a few minutes and the cost of a second occlude)[26] obviates the need for OAC for AF with its incessantly accruing bleeding risk, exponentially climbing with age. The term mechanical vaccination applies to PFO[7] and LAA[27] closure and both are oblivious to any compliance issue.

PART/4
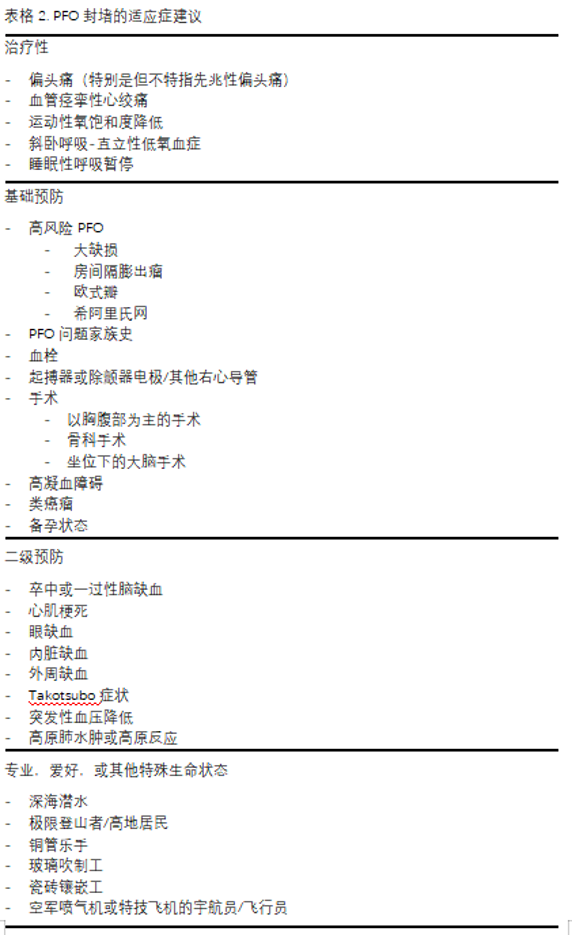
PFO封堵的绝对适应证(表格2)
目前,关于PFO封堵术预防缺血事件的随机对照数据仅限于60岁或65岁以下、发生脑缺血事件且除PFO外无其他明确病因的患者[28]。因此,所有指南均仅建议对此类患者进行PFO封堵术。将适应证推广到系统性循环中的其他栓塞事件、一级预防,或推广到年龄较大或有系统性栓塞其他潜在风险的患者,违背了循证医学(EBM)的原则。迄今为止,基于循证医学的指南无一例外地忽视了老年和体弱患者PFO相关事件的绝对风险更高这一事实[29]。无论出于什么样的年龄和情况,如果告知有风险的人群必须等到疾病相关事件第一次发生后才可以进行这种简单、无害又有效的预防手术,是一种冷酷并且可怕的行为。
At present, randomized data regarding PFO closure for ischemic events are limited to patients under the age of 60 or 65 years after a cerebral ischemic event with no findable putative cause other than the PFO [28]. As a consequence, PFO closure is exclusively recommended for such patients in all guidelines. To extrapolate indications to other embolic events in the systemic circulation, to primary prevention, or to patients who are older or have competing potential risks for systemic embolism breaches evidence-based medicine (EBM). Guidelines based on EBM so far inexcusably disregard that old and sick patients have a higher absolute risk of PFO-associated events [29]. Regardless of age and setting, it is cynical if not macabre to inform people at risk that they are to await a first event before this trivial, innocuous, and efficacious preventive procedure will be performed.
表格2列出了PFO封堵的合理适应证。这些都有数据进行支撑[30],尽管只对缺血性事件[31]和偏头痛[6]的随机对照实验有统计学意义,但比起实际地去收集数据,探索已有的随机对照实验数据难道不是更好?这已经是心脏病学中的最简单,却能够总体上产生最好的整体结果的手术。在对照组中,我们看到数不清的令人衰弱甚至致命的事件。这些事件在未来的随机对照实验中应该被规避,而不是仅仅观察并记录在研究表格中[29]。最重要的是,PFO封堵术的任何一种适应证的积极作用,都会带来其他所有适应证积极效果的附带益处。例如,由于偏头痛进行PFO封堵术后,患者相当于同时永久性的预防脑动脉、冠状动脉、眼动脉、内脏动脉或其他全身动脉的反常性栓塞。换句话说,PFO可以在发生任何栓塞事件后进行封堵,并且患者可能也会感受到偏头痛的痊愈。
Table 2 lists reasonable indications for PFO closure. They are all supported by data [30], albeit statistically significant in randomized trials only for ischemic events [31] and mi graine [6]. Yet are we and the patients not better off by extrapolating randomized data rather than actually collecting them with regard to cardiology’s simplest procedure that yields the best overall results considering positive minus negative aspects? The countless debilitating or even lethal events in control groups of future randomized trials can and should be prevented rather than just watched and marked down in study spreadsheets [29]. Most importantly, the positive aspects of any indication for PFO closure always bring about the positive effects of all other indications as collateral benefits. After a PFO closure for migraine, the patient is vaccinated permanently against paradoxical embolism into cerebral, coronary, ocular, visceral, or other systemic arteries. The other way around, a PFO can be closed after any embolic event and the patient may enjoy being cured from migraine.
4.1 治疗
偏头痛:偏头痛是治疗性PFO封堵的重要适应证。血管活性触发因子,主要是血清素,在肠道器官中产生,并在很大程度上被肺中和。如果大量静脉血通过PFO,体循环内会经历一次血清素海啸,这可能激活脑血管中的一个或几个超敏受体,导致皮质扩散性抑制 [32]。这种抑制等同于一次血管收缩,可能会激发出一次先兆性偏头痛并紧跟着发生反应性血管舒张,造成头痛。如果只有一个高度敏感的受体,头痛症状总是相同的。如果有多个高度敏感的受体,症状可能会有所不同。如果所有的过度反应触发受体都位于同一侧,那么症状可能仍然在同一侧。
Migraine: Migraine is the key indication for therapeutic PFO closure. Vasoactive triggers, foremost serotonin, are produced in the intestinal organs and become largely neutralized by the lung filter. If a gush of venous blood passes through a PFO, the systemic circulation experiences a serotonin tsunami that may activate one or several hyper-reactive receptors in the brain vessels, giving rise to a cortical spreading depression[32]. This corresponds to a transient vasoconstriction, possibly provoking an aura and being followed by reactive vasodilation causing a headache. In case of a single hypersensitive receptor, the migraine symptoms are always identical. With several hypersensitive receptors, symptoms may vary. They may still pertain to the same side in case all overreacting trigger receptors are located ipsilaterally.
然而,偏头痛为由的PFO封堵手术是循证医学被过度应用的另一个受害者,这对患者不利[29]。偏头痛人群中PFO的患病率和PFO人群中偏头痛的发生率都升高[33],这已经被证实,没有争议[34]。有一种根深蒂固的观点,特别是在神经学家中(但不仅限于他们),认为这可以用共同基因来解释。这种理论被PFO封堵能够缓解部分偏头痛的事实驳斥了。几乎所有的对比PFO伴偏头痛患者介入封堵和单纯药物治疗对照试验或随机对照试验中,PFO闭合后偏头痛显著改善。这在先兆性头痛中更为明显[35]。在大部分非随机性对照实验报告中,支持PFO闭合的不同观点有统计学意义[36,37]。在三个主要的随机对照实验中,尽管主要终点未达到预定的统计学显著性水平,但结果均倾向于PFO封堵术有利。大多数次要终点均显示PFO封堵术具有统计学上显著的优越性。纳入的偏头痛患者情况复杂,主要终点设定目标过于远大(大批量数据)且不幸失败(没有得出好结论)。并且,在有假手术过程的研究中,平衡假手术(安慰剂)效应导致了统计意义的缺失。证据医学被误用,即当优越性试验未能达到其主要终点时,这些试验被反复且错误地用来扼杀一项技术或一种化合物,尽管它们已证明具有非劣效性和数值上的优越性[29]。神经学协会错误地将 PFO封堵术排除在偏头痛药物治疗的替代或补充方案之外,尽管数据毫无疑问地表明,将 PFO封堵术作为偏头痛的治疗方案并不会对患者不利。事实上,它为患者提供了改善甚至治愈偏头痛的良好机会,更何况机械性疫苗接种作为一种简单安全的一次性措施,要优于长达一年的药物治疗。后者的费用和副作用即使不是终身的,也会持续数十年。
PFO closure in migraine is yet another deplorable victim of EBM applied overzealously to the disadvantage of patients [29]. An elevated prevalence of PFOs among migraine patients[33] and an elevated prevalence of migraine among people with a PFO are proved and uncontested [34]. An encrusted opinion prevails, particularly but not only among neurologists, that this is explainable by common genes. This theory is refuted by the fact that PFO closure improves some migraines. Almost all comparative or randomized trials investigating PFO device closure or medical treatment alone in patients with migraine showed a numerically conspicuous improvement of migraine with PFO closure. This was more pronounced in migraineurs with aura [35]. In most non-randomized comparative reports, the difference in favour of PFO closure was statistically significant [36,37]. In all three major randomized trials, the primary endpoints were favourable for PFO closure but failed the predefined statistical significance. Most secondary endpoints showed statistically significant superiority for device closure of the PFO. High complexity of the migraine patients included, overly ambitious and ill-fated primary endpoints, and, in the studies with sham procedures, the equalizing sham (placebo) effect contributed to the missed statistical significances. Misquoting EBM, superiority trials missing their primary endpoints are repeatedly and erroneously used to bury alive a technique or a compound despite proven non inferiority and numerical superiority[29]. Neurological societies mistakably exclude PFO closure as an alternative or supplement of drug treatment for migraine, although the data leave no doubt that it will not disadvantage patients to adopt PFO closure as a therapy option for migraine. In fact, it offers them a good chance of improvement, even cure, not to mention that a mechanical vaccination as a simple and safe one-time measure is preferable to year-long medical treatment. The latter accrues cost and side effects for decades if not for life.
神经科医生一直否认进行PFO封堵术对偏头痛患者的益处,再次忽视了对偏头痛患者进行PFO封堵术可带来的附带益处,即防止矛盾性栓塞、中风、心肌梗死甚至死亡。它还回避了随机试验[38](meta-analyses of randomized trials)中许多具有统计学意义的PFO封堵术的益处,甚至莫名其妙地回避了对单个患者数据进行的荟萃分析[6]。实际上,他们研究的所有结果都表明,PFO封堵术对偏头痛具有统计学意义上的显著优势。
The maintained denial by neurologists of a merit of PFO closure in patients with migraine once again neglects that PFO closure in patients with migraine carries along for free the collateral benefit of lifelong protection against paradoxical embolism, the likes of stroke, MI, or even death. It also scotomizes the many statistically significant benefits of PFO closure in meta-analyses of randomized trials [38], inexplicably even the ones performed on individual patient data[6]. Virtually all their examined endpoints depict statistically significant advantages of PFO closure in migraine.
对于患有典型偏头痛的患者,寻找PFO并对确诊的PFO进行封堵是值得的。至少有半数患者的偏头痛症状得到了及时和持续的改善,相当一部分患者甚至会永久痊愈,而且每一位患者都会因为已经永久封堵的PFO而受到保护,避免发生反常栓塞。
It pays out to search for a PFO in patients with typical migraine and close documented PFOs. At least half of such patients enjoy immediate and sustained improvement of migraine, a good percentage are even cured for good, and every single patient will be protected against paradoxical embolism through the PFO that is now closed for life.
一位39岁护士的病例令人十分不安,它充分体现了人们对偏头痛和PFO问题的态度。该患者因数十年难治性偏头痛转诊至我处。不幸的是,这发生在她因中风导致永久性失语两年多之后。我发现了一个PFO,并对其进行了经皮封堵术。偏头痛立刻消失了。如果她早几年来找我,当时就能克服致残性偏头痛。更重要的是,她就不会患上中风,也就不会在无法说话的情况下艰难地教育两个十几岁的儿子,以及在社会和职业上面临可怕的挣扎。
An utterly disturbing case vignette of a 39-year-old nurse exemplifies the unfortunate prevailing attitude to the migraine and PFO issue. The patient was referred to me for refractory migraine for decades. Unfortunately, this happened more than 2 years after she had been left permanently aphasic by a stroke. A PFO was found and percutaneously occluded. The migraine vanished instantly. Had she come to my attention years earlier, she would have overcome her disabling migraine at that time. More importantly, she would not have suffered the stroke and avoided the horrid struggle to educate two teenage sons and to function socially and professionally while being unable to speak.
血管痉挛性心绞痛:与偏头痛一样,血管痉挛性心绞痛也可能是由PFO通过的血清素浪潮导致的,在这种情况下可通过封堵PFO进行治疗[32]。即使血管痉挛性心绞痛没有缓解的患者也可以通过封堵的机械方法预防反常性栓塞。他们虽然没有得到疾病直接的改善,但却得到了间接的好处。
Vasospastic angina pectoris: Like migraine, vasospastic angina can be mediated by a PFOvia serotonin tsunamis and treated by PFO closure in such cases [32]. Even patients without improvement regarding vasospastic angina are mechanically vaccinated against paradoxical embolism. They lack the direct improvement but are recompensed by the collateral benefit.
运动性氧饱和度降低:一些人在剧烈运动时PFO持续开放,导致发绀并限制运动能力,从而出现运动性失饱和现象[39]。在50名患有PFO的所有患者中,有三分之一的人出现了这种现象[40]。PFO封堵后可改善大多数患者的情况,并保护所有患者避免日后发生矛盾性栓塞。
Exercise desaturation: Exercise desaturation occurs in some people when the PFO persistently opens during strenuous activities, causing cyanosis and limiting exercise capacity [39]. The phenomenon was documented in a third of 50 all-comers with a PFO [40]. PFOclosure improved it in most patients and protected all of them against later paradoxical embolism.
斜卧呼吸-直立性低血氧症:坐姿可能会使横膈膜向头颅方向扭曲,尤其是肥胖的老年人。这会影响心脏,使PFO打开并保持开放状态,直到体位改变。随之而来的是严重的动脉氧饱和度降低,这就是所谓的“直立性低氧血症”[39,41]。PFO封堵术解决了这一问题,并避免了此类患者伴随的血栓反常性栓塞的风险。
Platypnea orthodeoxia: The sitting position may distort the diaphragm cranially, especially in the obese elderly. This impacts the heart in a way that the PFO opens and stays patent until the body position is changed. Significant arterial desaturation ensues and is called platypnea orthodeoxia [39,41]. PFO closure solves that and does away with the accompanying high risk of paradoxical embolism of thrombi of such patients.
睡眠呼吸暂停综合症:睡眠呼吸暂停分为阻塞型和中枢型两种[42]。阻塞型睡眠呼吸暂停会因为延长的吸气阶段导致静脉回流至胸腔的血量增加。通常会导致PFO开放。这增加了发生反常性栓塞的风险,同时,由于开放的PFO会加重氧饱和度降低,从而使中枢性睡眠呼吸暂停恶化[43-45]。封堵PFO可以改善所有这些情况。
Sleep apnea: Thera are obstructive or central forms of sleep apnea [42]. The obstructive type causes increased venous backflow into the chest during extended inspiration phases. A PFO is often opened by that. This increases the risk of paradoxical embolism and, at the same time, worsens central sleep apnea because the open PFO aggravates oxygen desaturation [43–45]. PFO closure improves all that.
4.2 一级预防
现在是将PFO封堵术用于一级预防提上日程的时候了。第一步可能先仅限于已知患有高风险 PFO 的人群。
It is high time to place PFO closure for primary prevention on the agenda. In a first step, it may stay limited to people who happen to be known to have a high-risk PFO.
高危PFO:顺带一提,“高危”这一标签可用于所有假定已导致缺血事件并考虑进行二级预防的PFO。对于一级预防,高危PFO是指那些具有高危解剖和生理特征的PFO。它们是大型PFO、自发性右向左分流的 PFO,以及与房间隔膨出瘤(简称 ASA[8])、欧氏瓣[9-12]或希阿里氏网[13]相关的PFO。ASA几乎每次心跳都会打开PFO,因此右向左分流的总体时间相当长。欧氏瓣或希阿里氏网使得下腔静脉流入的血栓(几乎所有血栓都来自下腔静脉)直接通过PFO。所有这些解剖变异都与PFO的发病率增加有关。它们是先天性的,出生后会阻碍PFO闭合。
High-risk PFO: As a side note, the label ‘high-risk’ can well be employed for all PFOs presumed to have already caused an ischemic event and are considered for secondary prevention. For primary prevention, high-risk PFOs are those with high-risk anatomical and physiological features. They are large PFOs, PFOs with a spontaneous right-to-left shunt, and PFOs associated with a hypermobile septum primum, referred to as ASA [8], a Eustachian valve [9–12], or a Chiari network [13]. An ASA opens the PFO with practically every heartbeat, thereby accruing considerable overall time with a right-to-left shunt. The Eustachian valve or the Chiari network escorts the clots from the inflow of the inferior vena cava (virtually all thrombi come from there) directly through the PFO. All these anatomical variations are associated with an increased prevalence of a PFO. They are congenital and hinder PFO closure after birth.
有PFO问题的家族史:有一个或多个近亲属(如双胞胎)曾发生过由PFO引起的中风、心肌梗死或其他缺血性事故,或在PFO封堵术后偏头痛有所改善,这些人是PFO封堵术用于一级预防的额外候选者。
Family history of PFO problems: People with one or more close blood relatives, e.g., a twin, having suffered a PFO-mediated stroke, MI, or other ischemic accident, or having experienced improvement of migraine after PFO closure, represent additional candidates for PFO closure for primary prevention.
血栓栓塞或高凝血障碍:有血栓栓塞病史或高凝状态[46]的患者,即使长期使用OAC,也应接受原发性PFO封堵治疗[47]。OAC的依从性问题众所周知,而且会出现医学上强加的暂停。PFO封堵术既不存在依从性问题,也不存在暂停问题。
Thromboembolism or hypercoagulable blood disorders: Patients with a history of thromboembolism or with hypercoagulability [46] should be offered primary PFO clo sure [47], even if they are under chronic OAC. OAC is notorious for compliance problems and there are medically imposed pauses. PFO closure knows neither compliance issues nor pauses.
起搏器,除颤器电极、其他右心导管或腔静脉过滤器:静脉循环中的所有异物都是潜在的血栓栓塞源,会增加PFO患者发生矛盾性栓塞的危险。腔静脉过滤器也是如此。它们能阻挡大血栓,但不能阻挡PFO介导的典型全身性栓塞的小血栓。事实上,它们本身就是小栓子的潜在病灶。
Pacemaker or defibrillator electrodes, other right heart catheters, or vena cava filter: All foreign bodies in the venous circulation are potential sources of thromboembolism and place PFO carriers at increased jeopardy for paradoxical embolism. This also holds true for vena cava filters. They block large clots but not the small clots typical of PFO-mediated systemic embolism. In fact, they, themselves, constitute a potential nidus for small emboli.
重大手术:如果时间允许,接受重大手术治疗的患者应接受PFO筛查。然后应在手术前关闭PFO[48]。这可将术后第一年内发生中风的风险从9%降至1%。神经外科医生在为采取坐位以减少重力导致的静脉出血的患者进行手术时,应确保没有(未闭合的)PFO[49]。手术中打开的脑静脉容易吸入空气,这些空气有可能通过PFO绕过肺部过滤器,最终进入全身循环。由于空气比血液轻,因此往往会倾向于上升到脑部,即坐位患者的最高器官。
Major surgery: Time permitting, patients undergoing major surgical interventions ought to be screened for a PFO. PFO closure should then precede surgery [48]. It reduces the risk of a stroke from 9% to 1% within the first year after surgery. Neurosurgeons operating on sitting patients in order to reduce venous bleeds depending on gravity should make sure that there is no (unclosed) PFO [49]. Brain veins that are opened during surgery have a propensity to catch air that risks bypassing the lung filter through a PFO to end up in the systemic circulation. Being lighter than blood, air will tend to climb to the brain, the topmost organ of the sitting patient.
类癌瘤:类癌肿瘤引起的左心瓣膜问题在PFO患者中更为常见[50]。这些肿瘤通常会产生足以损害心脏瓣膜的高剂量血清素。如果血清素能够绕过肺部的生理中和作用,瓣膜的损伤不仅涉及右心,还涉及左心。临床上,左心瓣膜的破坏性更大。封堵PFO可以防止这种情况发生。
Carcinoid tumour: Left heart valve problems with carcinoid tumours are more com monif the patients have a PFO [50]. These tumours typically produce serotonin in high enough doses to damage heart valves. In case the serotonin can shortcut the physiological neutralization during the lung passage, valve destruction not only pertains to the right but also to the left heart. There, it is clinically more devastating. PFO closure prevents that.
备孕:怀孕会增加血栓形成的风险,并导致右心房压力升高。这增加了PFO的潜在危害性。虽然只有传闻,没有可靠的数据证明PFO的存在会增加妊娠风险[51,52],但考虑到附带的益处,在计划妊娠前关闭PFO是无可厚非的。
Planned pregnancy: Pregnancy is associated with an increased risk of thromboem bolism and a rise in right atrial pressure. This enhances the deleterious potential of a PFO. Although there are only anecdotal and no robust data to prove that the pregnancy risk be increased by the presence of a PFO [51,52], closing a PFO before a planned pregnancy cannot be wrong, considering the collateral benefits.
4.3 二级预防
中风和短暂性脑缺血发作(TIA):栓塞性脑卒中与栓塞性TIA的区别仅在于症状的不可逆性,发生哪个取决于运气。两者在PFO筛查和封堵的适应证上不应有任何区别。TIA的症状可能与偏头痛相似。特别是在这种情况下,PFO封堵术是治疗偏头痛的一种重要方法,并可防止未来发生真正的栓塞性中风,是首选的干预措施。对于疑似栓塞性脑卒中的患者,不能以存在其他潜在的卒中原因或患者年老或有合并症为由而不封堵PFO。与相对收益不同,PFO封堵术的绝对收益率随患者年龄和疾病的增加而增加。与老年人和有疾病的人相比,年轻人和所谓的隐源性卒中患者发生由PFO介导的反常性栓塞的风险较低。房颤也不是PFO封堵术的禁忌症。即使在使用口服抗凝药物(OAC)的情况下,PFO关闭也是有益的。心房颤动比无心房颤动时更容易发生反常性栓塞,因为静脉循环中有更多的血凝块。对年轻且其他方面健康、发生脑卒中的患者进行隐匿性AF的广泛筛查意义不大,其结果可以忽略不计。即使检测出房颤,它也不太可能是疾病发生的罪魁祸首。高风险的PFO与房颤相比更有可能是罪魁祸首。此外,冗长的房颤搜索会推迟甚至遗忘最初计划的PFO封堵术。为此,代价是众多可预防但未预防的PFO事件。最后,一个明显而有吸引力的方法是同时关闭PFO和LAA。这不仅终止了OAC的适应证,还能延长两倍的寿命。与华法林[53]或新型口服抗凝药[54]相比,PFO封堵术[22]和LAA封堵术均显示出生存获益。
Stroke and transient ischemic attack (TIA): An embolic stroke differs from an embolic TIA only in the irreversibility of symptoms, which is subject to chance. No differences should be made in the indications for PFO screening and closure between the two. TIA symptoms may be mimicked by migraine. Especially in such cases, PFO closure, being a valuable therapy for migraine and protecting against future real embolic strokes, is the intervention of choice. The PFO cannot be acquitted in patients with a cerebral event presumed to be embolic on the basis that there are other potential stroke causes or because the patient is old or has comorbidities. The absolute yield, in contrast to the relative yield, to be expected with PFO closure, increases with the age and disease of the candidates. Compared to the old and sick, the young and so-called cryptogenic stroke patients have a lower risk of a PFO-mediated paradoxical embolism. AF is not a contra-indication to PFO closure, either. Even under OAC, PFO closure is beneficial. Paradoxical embolism is more common with AF than without, as there are more clots in the venous circulation, and it is fully preventable by PFO closure but only partially by OAC. Extended screening for occult AF in young, otherwise healthy patients with a cerebral accident makes little sense. The yield is negligible. Even if AF is detected, it is unlikely that it was responsible for the event. Ahigh-risk PFO is a much more likely culprit. In addition, a lengthy search for AF defers or even makes the initially planned PFO closure forgotten about. Additional preventable yet un-prevented PFO-mediated events may be the price for that. Finally, an obvious and attractive approach is to simultaneously close the PFO and the LAA. This puts an end to the indication for OAC and improves longevity twofold. Both PFO closure [22] and LAA closure—compared to warfarin [53] or to novel oral anticoagulants [54]—have shown a survival benefit.
心肌梗死:经PFO导致的反常栓塞引起的心肌梗死,一定是心脏病学中最常见的误诊问题之一[55]。这一点尤其令人头疼,因为只要关闭PFO就能轻松预防。这种疏忽应归咎于心脏病专家。神经科医生出于模糊不清的原因,希望在检查PFO之前排除所有其他可能导致中风的原因,有了神经科医生的坏榜样,心脏病专家在考虑反常性栓塞之前就会想到所有可能导致心肌梗死的原因。如果没有明显的动脉粥样硬化(首要嫌疑人),自发性冠状动脉夹层、长期痉挛或药物滥用都会被考虑,但不考虑PFO。被忽视的事实是,动脉粥样硬化、年龄和全身性疾病会促进而非排除静脉血栓的反常性栓塞。只有少数介入心脏病专家将PFO列为心肌梗死的公认病因之一。静息时,冠状动脉的供血量约为220毫升/分钟。这几乎相当于大脑供血量(约750毫升/分钟)的三分之一。通常通过PFO的小血块会对这两个器官造成同样的危害。四肢和内脏器官需要更大的血栓才能造成严重的缺血性伤害。在大脑和心脏中,由于存在非重点区域、预先存在的组织疤痕或侧支区域,会出现无症状栓塞。考虑到所有这些因素,大约每三次脑部事件中就有一次心肌梗死,这些都归功于PFO。神经内科对PFO引起的脑事件的诊断严重不足,这一点尚未引起重视。通常情况下,风险最高的患者会被默认排除。被正确诊断为PFO导致的心肌梗死的人数至少应比目前高出数百倍。一旦冠状动脉情况得到控制,任何急性心肌梗死哪怕看起来只有一点栓塞的迹象,都应立即查找PFO。这可以通过在初级冠状动脉经皮介入治疗结束后进行右心导管检查来实现。比起像上所述用导丝导管直接探查PFO,右心房注射或许会更好(图 1)。有一个很小但令人担忧的风险,即血栓栓塞在PFO上[24],部分血栓脱落导致急性心肌梗死。以这种方式排除或证明并封堵PFO只需几分钟,而且无论白天还是黑夜都可以进行。这种方法并不会增加手术的整体风险,但却有很多好处。对于栓塞性心肌梗死,无论其是否确实由PFO引起,这种方法都是有意义的,因为下一次心肌梗死很可能就是由PFO引起的。针对反常性栓塞的预防性机械疫苗永远不会毫无根据。顺便说一句,与TEE相比,使用右心导管筛查PFO不会让患者感到不适。在使用造影剂(图1)进行此类检查时,可以同样清楚地描绘出在选择合适的装置尺寸时需要注意的PFO特征(图4)。联合冠状动脉介入治疗和PFO封堵术符合患者的利益。
MI: MIbyparadoxical embolism through a PFO must be one of the most frequently misdiagnosed problems in cardiology [55]. This is particularly vexing because it is easily preventable by PFO closure. The cardiologists are the ones to blame for this oversight. In the wake of the bad example of neurologists, who, for nebulous reasons, want to have excluded all other putative causes for stroke before scouting for a PFO, cardiologists think of all imaginable causes of an MI before considering paradoxical embolism. In the absence of obvious atherosclerosis (the prime suspect), spontaneous coronary dissection, protracted spasm, or drug abuse are pondered, searched for, or incriminated right off the bat, but not a PFO. The mentioned fact goes ignored that atherosclerosis, age, and systemic disorders promote rather than exclude paradoxical embolism of a venous clot. Only a minority of interventional cardiologists list a PFO among the acknowledged causes of MI. The amount of blood supply to the coronary arteries is about 220 mL/minute at rest. This corresponds to almost a third of that to the brain (roughly 750 mL/minute). Both organs are equally jeopardized by the small clots typically passing through a PFO. Limbs and visceral organs require larger clots for serious ischemic harm. In the brain and heart, there are silent embolisms thanks to unimportant areas, pre-existing tissue scars, or collateralized territories. Accounting for all that, one should attribute to a PFO roughly one MI per three cerebral events. It has not yet been taken into account that neurology significantly underdiagnoses PFO-mediated cerebral events. Typically, they are ruled out by default in patients with the highest respective risk. The number of correctly diagnosed PFO-mediated MIs should probably be at least hundredfold higher than it currently is. Anyacute MI looking even remotely embolic should prompt a search for a PFO, once the coronary situation is managed. This can be accomplished with a right heart catheterization at the end of the primary coronary percutaneous intervention. Rather than directly probing the PFO with a wire or a catheter as described above, a right atrial injection is preferable (Figure 1). There is a small but concerning risk of a thrombus saddling the PFO [24], part of which just broke off and caused the acute MI. Excluding or proving and closing a PFO in that way adds a few minutes to the coronary case and is doable day or night. It does not really increase the overall risk of the procedure but can do a lot of good. It makes sense in embolic-looking MIs irrespective of whether or not they were indeed caused by the PFO. The next MI could well be, and a mechanical vaccination against paradoxical embolism is never unwarranted. By the way, screening for a PFO with a right heart catheter is less uncomfortable for the patient than with a TEE. The features of the PFO to be respected when selecting the appropriate device size (Figure 4) can be equally well depicted in such a study with contrast medium (Figure 1). A combined coronary intervention and PFO closure is in the vetted interest of patients.
眼部、内脏或外周缺血,Takotsubo事件,突发性低血压,高海拔肺水肿或高山反应: PFO与眼部、内脏或外周栓塞的致病关系与脑部和冠状动脉缺血事件的致病关系相同。然而,除眼部栓塞外,更大的血栓非常危险。它们不太可能通过普通的PFO。PFO可能通过与上述偏头痛或血管痉挛性心绞痛类似的机制引发takotsubo事件。突发低血压和高海拔肺水肿或高山症与PFO的关系将在下文中阐述。
Ocular, visceral, or peripheral ischemia, takotsubo events, decompression accidents, and high-altitude pulmonary edema or mountain sickness: The causative relationship of the PFO with ocular, visceral, or peripheral embolism is the same as that of cerebral and coronary ischemic events. Yet, with the exception of ocular embolism, larger clots are at stake. They are less likely to pass a regular PFO. A takotsubo event may be triggered by a PFO via a mechanism similar to the one described above for migraine or vasospastic angina pectoris. Decompression accidents and high-altitude pulmonary edema or mountain sickness in the realm of PFOs are dealt with in the paragraphs below.
4.4 专业,爱好和其他特殊生命情况
深海潜水员:潜水有减压病的风险,主要是氮气气泡导致。静脉循环中较多的气泡会被肺过滤器排出。PFO会大大增加这些气泡绕过过滤器到达大脑等敏感器官的风险[56]。如果存在PFO,潜水员更容易发生脑部事件,磁共振成像上的脑裂隙病变就是证明[57]。封堵PFO 可有效防止进一步的减压病[56]。
Deep sea divers: Diving carries a risk for decompression accidents, mainly by nitrogen bubbles. The more prevalent ones in the venous circulation are eliminated by the lung filter. A PFO increases the risk significantly that such bubbles bypass the filter to reach sensitive organs like the brain [56]. Divers more commonly suffer cerebral events, as evidenced by lacunar brain lesions on magnetic resonance imaging, if they have a PFO [57]. PFO closure works well for preventing further decompression events [56].
极限登山者或高原居民:高海拔脑水肿和肺水肿(又称急性登山病)在患有PFO的人中更为常见 [58,59]。关闭PFO可以预防或纠正这种情况。这肯定会改善整体预后。众所周知,高原反应会导致右心房压力长期升高。由于环境空气中的氧气浓度较低,肺动脉会收缩,从而减缓血液通过肺部的速度,促进氧气向红细胞的转移。右心房压力升高会导致类似Valsalva动作呼气状态下的情况持续存在,并可能使PFO保持开放。患有PFO的高地居民发生反常性栓塞的风险大大增加。他们可能会通过PFO出现永久性的右向左分流,进一步降低血液中的氧饱和度,导致肺动脉血管收缩加剧,从而使情况恶化。右心房压力进一步升高,恶性循环继续进行。
Extreme mountain climbers or highlanders: High-altitude cerebral and pulmonary edema, also known as acute mountain sickness, is more common in people with a PFO [58,59]. PFO closure deserves a chance to prevent or remedy that. It will improve the overall prognosis, for sure. Highlanders are known to develop chronic elevated right atrial pressures. Constriction of pulmonary arterioles occurs, secondary to low oxygen concentrations of ambient air, to slow down blood passage through the lungs for facilitating oxygen transfer to the red blood cells. Elevated right atrial pressure perpetuates a situation similar to that at the release of a Valsalva maneuver and may keep a PFOopen. Highlanders with a PFO are at a substantially increased risk for paradoxical embolism. They may experience a permanent right-to-left shunt through the PFO that deteriorates the situation by further decreasing oxygen saturation in the blood and leading to additional pulmonary arterial vasoconstriction. The right atrial pressure increases further and the vicious cycle goes on.
铜管乐手、玻璃吹制工或瓷砖镶嵌工:铜管乐手和玻璃吹制工在工作时会做Valsalva动作。在PFO尚未得到治疗的情况下进行蹲姿活动,容易导致氧饱和度降低和反常性栓塞。
Brass musicians, glass blowers, or tile setters: Brass musicians and glass blowers use Valsalva maneuvers for work. Activities in crouching positions with a not-yet-treated PFO render one prone to oxygen desaturation and paradoxical embolism.
宇航员、空军喷气式飞机或杂技飞机的飞行员:高加速度会给PFO携带者带来发生反常性栓塞的风险,但仅限于PFO封堵之前。
Astronauts or pilots of air force jets or acrobat planes: High accelerations represent a risk for paradoxical embolism in PFO carriers, but only until the PFO is occluded.
PART/5
概要
PFO很可能是被低估、研究不足、治疗上被忽视的心血管健康隐患。具有讽刺意味的是,在心脏病的所有危险因素和疾病中,它是最容易消除的。PFO介入封堵术是介入心脏病学中最简单、最无害的手术,也可能是总体效果最好的手术,被称为机械疫苗,因为它主要是一种预防性干预措施。尽管如此,对于很大一部分PFO患者来说,PFO封堵术在治疗PFO相关症状方面是有效的。当关闭PFO以预防与PFO相关的问题(如缺血性脑、冠状动脉、眼、内脏或外周反常性栓塞)时,可带来额外的收益,如改善PFO引起的偏头痛、运动不耐受等。出于其中一个原因关闭PFO,也会一同确切地消除了所有其他与PFO相关的问题。
The PFO may well top the list of underestimated, poorly worked up, and therapeutically neglected cardiovascular health hazards. Ironically, among all risk factors and medical problems in cardiology, it is the easiest to remove. PFO device closure, the most simple and innocuous procedure of interventional cardiology with likely the best overall yield, is referred to as a mechanical vaccination as it is predominantly a preventive intervention. Notwithstanding, PFO closure is therapeutically effective regarding PFO-related symptoms in a significant proportion of PFO carriers. A collateral benefit can be expected when closing a PFO to prevent a PFO-related problem, such as ischemic cerebral, coronary, ocular, visceral, or peripheral paradoxical embolism, in terms of improvement of PFO-induced migraine, exercise intolerance, etc., and vice versa. Close a PFO for one reason and you have eliminated all other PFO-related problems for free and for sure.
约有25%的人口存在PFO,其中约有5%的人存在特别危险的PFO。至少在后一类人群中,筛查并封堵PFO作为一级预防似乎更有优势和成本效益。
A PFO exists in perhaps 25% of the population, with its particularly dangerous forms in presumably 5%. Screening for and closure of the PFO as primary prevention appears advantageous and cost-effective in at least the latter group.
现在是时候在指南和教科书中将PFO列为任何可能导致栓塞的缺血性脑部、冠状动脉或其他全身性疾病的重要候选病因了,尤其是在高龄或有其他并发症的人群中。PFO只适用于健康、年轻且怀疑有矛盾性栓塞的患者,这种常见的说法必须彻底打破:患者的病情越重、年龄越大,静脉血栓的发病率就越高,因此PFO导致栓塞事件的概率也就越高。因此,与PFO相关的栓塞性心肌梗死比目前判断出的疑似病例要常见得多,更不用说诊断了,尤其是在老年人和病人中。根据生理系统血液分布情况,每三个脑栓塞中,就有一个冠状动脉栓塞。
It is high time to list the PFO in guidelines and textbooks as a serious candidate culprit for any ischemic cerebral, coronary, or other systemic event that could be embolic, particularly in people of age or with comorbidities. The common myth that a PFO is only to be looked for in otherwise healthy and young patients with suspicion of paradoxical embolism must be laid to rest once and for all: the sicker and older the patient, the higher the prevalence of venous thrombosis and, thus, the higher the absolute probability that the PFO causes an embolic event. Along these lines, PFO-related embolic MIs are much more common than currently suspected, let alone diagnosed, especially in old and sick people. For every three emboli finding the brain, one will find a coronary artery based on the physiological systemic blood distribution.
几乎没有人会为封堵PFO而后悔;更有可能的是后悔没有封堵PFO。
Hardly will one ever regret having closed a PFO; much more likely will one regret not having closed a PFO.
在PFO封堵前等待首次PFO相关症状发生是不安全的。它可能是致命的,也可能留下不可逆转的临床破坏性损害。
It is not safe to await the first event before PFO closure. It may be fatal or leave behind irreversible and clinically devastating damage.
房颤不是PFO封堵术的重要不良反应。PFO封堵术后的房颤只发生在房颤已经迫在眉睫的患者身上,是一种临床事件需要治疗。由于存在依从性问题和必要时候的停药,可能或有必要使用的长期OAC不能完全防止血栓栓塞。PFO封堵术是对OAC的补充。它既不会出现依从性问题,也不会因为任何原因暂停效益,而且不会引起出血问题。
AF is not an important adverse effect of PFO closure. AF after PFO closure only occurs—in a form that is clinically relevant and needs treatment—in patients in whom AF was already imminent before. Chronic OAC that might be or become necessary because of pre-existing or new AF or a coagulation disorder provides incomplete protection against thromboembolism because of compliance problems and imposed pauses. PFO closure supplements OAC. It knows neither compliance issues nor pauses, and it causes no bleeding problems.
封堵PFO并不会使后续的左心房导管介入(如房颤消融、LAA关闭或二尖瓣介入)变得更加复杂。相反,可显影的PFO封堵器一般会在其尾部划定了一个安全区域,方便在透视引导下对房间隔进行穿刺(图3)[60]。
PFO closure will not render more intricate subsequent left atrial access for catheter based interventions such as ablation for AF, LAA closure, or mitral valve interventions. On the contrary, a visible PFO occluder delineates, just caudal to it, a safe area for fluoroscopically guided transseptal puncture of the septum primum (Figure 3) [60].
<上下滑动查看更多>
资助:本研究未获得外部资助。
机构审查委员会声明:无需。
知情同意声明:无需。
数据可用性声明:无需。
数据可用性声明:不适用。
Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: Not applicable.
Data Availability Statement: Not applicable.
Conflicts of Interest: The author declares no conflicts of interest
免责声明/出版商说明:所有出版物中包含的声明、观点和数据仅代表作者个人和撰稿人的观点,与 MDPI 和/或编辑无关。MDPI 和/或编辑不对内容中提及的任何观点、方法、说明或产品造成的人员或财产损失承担责任。
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content
*医学上面无绝对,本文仅代表文献本身观点

扫码观看可降解学苑精彩内容
关注我们
专业的心血管医生学术交流平台

点击关注

点击下载
版权及免责声明:
本网站所发表内容知识产权归属医谱平台、主办方以及原作者等相关权利人,未经许可,禁止进行复制、传播、展示、镜像、转载、摘编等。经授权使用,须注明来源,否则将追究其法律责任。有关作品内容、版权和其他问题请与本网联系。
发表留言
暂无留言
输入您的留言参与专家互动