Breakthroughs in Heart intervention: Highlights from TEER MDT Webinar

On June 11, 2024, the TEER MDT webniar hosted by West China Hospital & Mount Sinai Heart Center proceeded smoothly online as scheduled. Professors Mao Chen and Yuan Feng from West China Hospital, Sichuan University, presented a case of Mitral Transcatheter Edge-to-Edge Repair (M-TEER) surgery in a patient with Degenerative Mitral Regurgitation (DMR) accompanied by calcification in the target area. During the procedure, aided by 3D and ultrasound guidance, two MitraClip™ XTR valve clips were successfully deployed, resulting in no residual regurgitation of the mitral valve and an average transvalvular pressure gradient of less than 4mmHg postoperatively.
Subsequently, Prof Gilbert Tang from Mount Sinai Heart Center shared two highly instructive cases of M-TEER surgery: one involving M-TEER following failure of surgical "Alfieri Stitch" repair technique, and the other concerning re-M-TEER for recurrent Mitral Regurgitation (MR) post initial M-TEER. Both cases underscored the importance of meticulous assessment of anatomical structures such as leaflet integrity, length, and width after the first surgery.
West China Hospital
Patient Information: A 75-year-old male patient presented with exertional dyspnea and chest tightness. He had a history of persistent atrial fibrillation and hypertension. Ultrasonographic evaluation revealed the following: LVEDD 55mm, LVESD 35mm, LA 42mm, LVEF 66%; moderate Aortic Regurgitation (VC=5mm), mild to moderate Tricuspid Regurgitation, PASP 25mmHg; severe Mitral Regurgitation (Carpentier Type II), VC=10×6mm; Mitral Valve Prolapse (A2 and A3), with a leaflet width of 11mm; Mitral Valve thickening, with calcification at the base of P2; Mitral Valve Area 6.2cm2; MV leaflet lengths: A2 26mm, P2 10mm (7.5mm without calcification).
Preoperative ECG
Preoperative TTE

Left: Mild to moderate TR Right: Moderate AR
LVOT View
Bicuspid Mitral Valve View
X-Plane
3D View
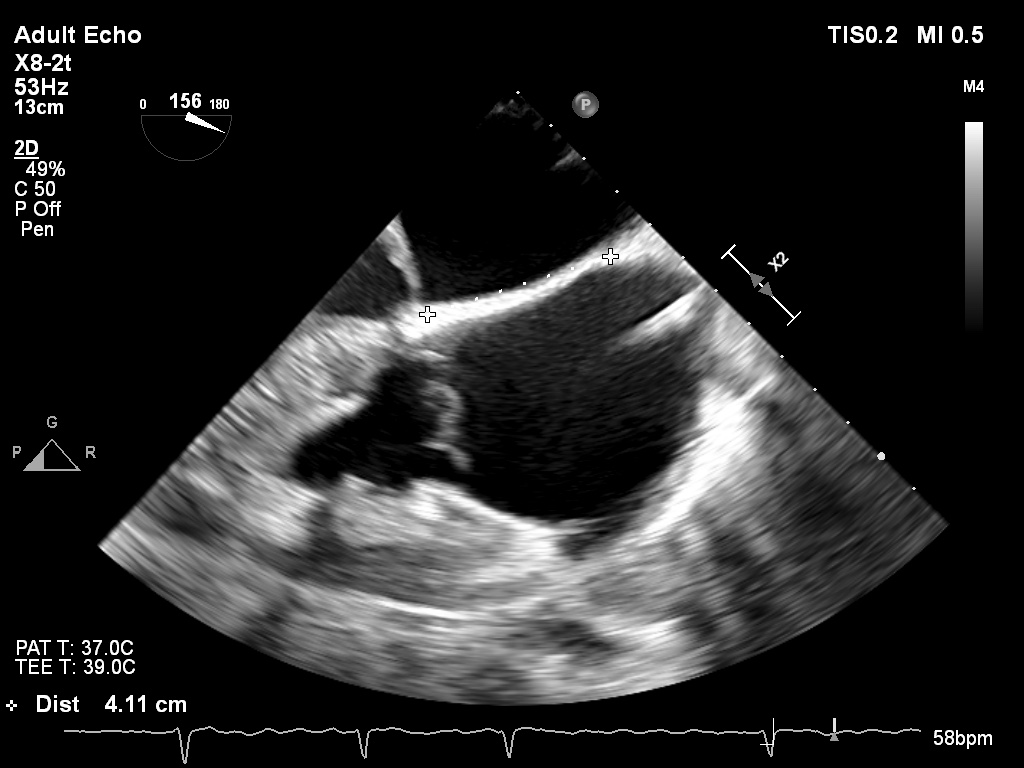
Puncture Depth:4.11cm
Preoperative Discussion: The width of the anterior leaflet at 11mm and the calcification at the base of P2 present challenging issues in this patient. In the scenario of surgical intervention, addressing the issue of the anterior leaflet width would be necessary. However, for a TEER procedure, the calcification indeed poses concerns. Given that the MitraClip™ XTR arms are 12mm in length, they seem suitable for the calcification and long leaflet situation in this patient. If opting for the NTR clip, as its arms are 9mm in length, the challenge lies in ensuring proper grasping of the true leaflet and not the prolapsed one, to prevent Single Leaflet Device Attachment (SLDA) and clip detachment risks.
Procedure: Following successful septal puncture, the first MitraClip™ XTR was implanted. With the aid of ultrasound and three-dimensional adjustments, the clip was positioned close to the A1P1 region in the A2-P2 area and successfully closed. Subsequent assessment via 3D views and X-Plane revealed leaflet prolapse in the A2-A3 region after the implantation of the first clip. After team discussion, it was decided to implant the second XTR clip in this region near the position of the first clip, while avoiding the area of calcification in the P2 region. Ultimately, the process of grasping the leaflet and closure was smoothly completed for the second clip as well. Following the implantation of both clips, both biplane and 3D views demonstrated no mitral regurgitation, with an average transvalvular pressure gradient of less than 4mmHg.
The process of implanting the first clip
The positioning of the first clip
The leaflet grasping process
The closure of the clip
3D view after the implantation of the first clip
X-Plane view after the implantation of the first clip
The process of implanting the second clip
The positioning of the second clip

Left: The leaflet grasping process Right:The closure of the clip
The biplane view obtained after the implantation of both clips
The 3D view after the implantation of both clips
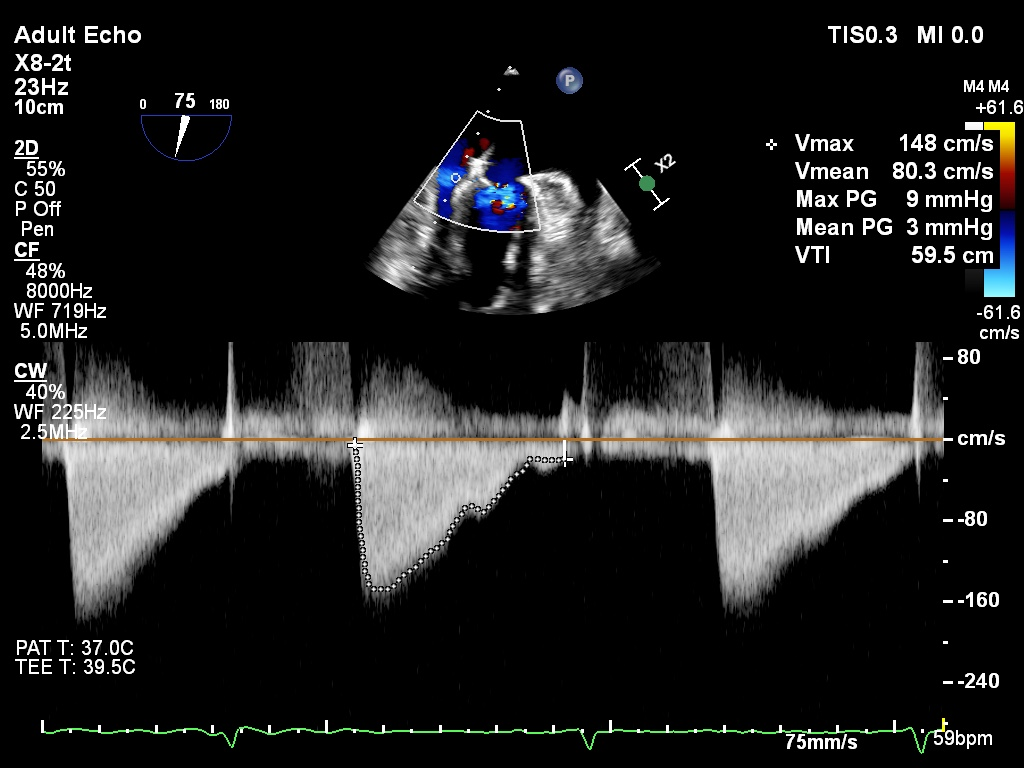
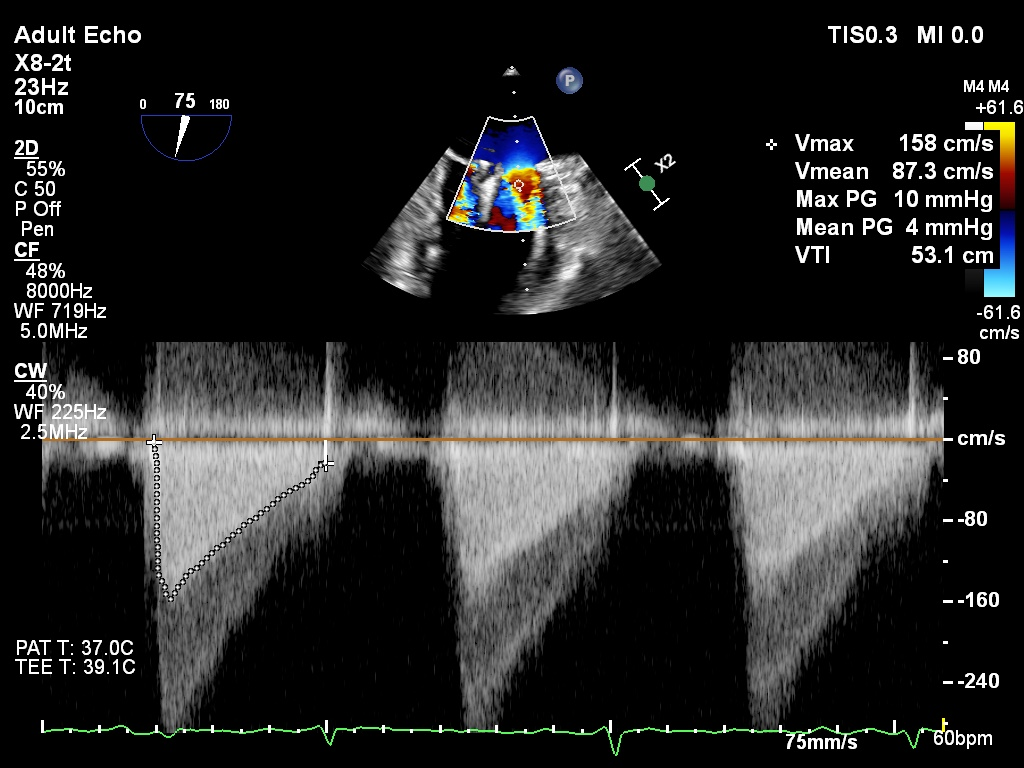
The average transvalvular pressure gradient
Discussion
Professor Mao Chen: In this surgery, we considered both long-term durability and safety, opting for two XTR clips instead of one wider clip. Given the calcification at the base of the P2 region, we ensured that the positions of the two clips were relatively close, side by side, to avoid any reflux between them. Therefore, real-time ultrasound assessment during the procedure provided excellent guidance and ultimately helped us achieve a good postoperative outcome.
Professor Gilbert Tang: Generally, the A2-P2 region is the most ideal position for clipping. However, clinically, approximately one-third of patients with regurgitation exhibit it from other areas, known as non-central MR. For non-central MR clipping, especially involving the leaflet coaptation area, higher demands are placed on clipping procedures, including the location of the septal puncture point (crucial), imaging assessment (3D-TEE), and instrument selection (the presence of numerous tendinous cords in the leaflet coaptation area makes it easier for longer grippers like XTR/XTW to entangle and damage them, but choosing NTR/NTW may result in insufficient grasping of the leaflets, necessitating a balance between the two).
Mount Sinai Heart Center
Patient Information: A 73-year-old male patient presented with intermittent dizziness and leg edema. Cardiac ultrasound revealed a torn posterior leaflet of the mitral valve with severe Mitral Regurgitation (MR). He has a history of complex mitral valve repair surgery. In October 2023, he underwent mitral valve "Alfieri Stitch" procedure, tricuspid valve repair, and left atrial appendage closure. He has a past medical history of Heart Failure with Reduced Ejection Fraction (HFrEF) with a Left Ventricular Ejection Fraction (LVEF) of 40%. During this follow-up, Transthoracic Echocardiography (TTE) revealed severe MR status post-surgery.
Preoperative TEE

Preoperative 3D View
Preoperative X-Plane
Strategy and Procedure:
Given the patient's high surgical risk for redo surgery (STS score 16.8%), the decision was made to opt for MitraClip™ Edge-to-Edge Repair (M-TEER). The plan involved placing a MitraClip™ G4 NT clip adjacent to the "Alfieri Stitch" during the surgery. Under 3D guidance, the subvalvular position was confirmed, followed by leaflet grasping. Bouncing was observed, indicating proper engagement, and the clip was slowly closed. Postoperatively, assessment revealed both leaflets were well seated with tissue bridges observed on 3D imaging. Moreover, there was a significant reduction in mitral valve regurgitation to trace amounts, with an average transvalvular pressure gradient of 5mmHg.
The positioning of the clip
Left: Independent grasping of the anterior leaflet
Middle: Embedding of the leaflets and bouncing observed during the procedure.
Right: Closure of the clip.
The evaluation of the clip
Postoperatively, there was trace regurgitation observed, with an average transvalvular pressure gradient of 5mmHg.
Discussion
Professor Gilbert Tang: For patients experiencing recurrent MR after surgical intervention, careful assessment of the risks and benefits of a redo surgery is essential. The technical challenges associated with redo surgery cannot be overlooked. Therefore, finding safer and more effective alternative strategies is crucial. Transcatheter Edge-to-Edge Repair (TEER), as an innovative surgical approach, offers new treatment options for such patients. It stabilizes previous repairs, reducing or eliminating the need for valve replacement, thereby lowering surgical risks and improving patients' quality of life.
However, although a small annulus does not necessarily constitute an absolute contraindication to TEER surgery, we must fully consider the impact of previous valve surgeries on the anatomy of the mitral valve, as well as the potential issue of mitral valve gradients. The width of the regurgitation and residual tissue play crucial roles in predicting postoperative mitral valve gradients. Therefore, detailed imaging examinations and assessments are necessary before surgery to ensure the safety and effectiveness of the procedure.
Professor Mao Chen: There is no doubt that the surgical risk for this case is relatively high. For such patients, collaboration among multidisciplinary teams is crucial. Doctors from departments such as cardiovascular surgery, cardiology, and imaging need to discuss together to develop personalized surgical plans. Close monitoring of the patient's condition during surgery is essential to ensure its success. In practical work, only by comprehensively considering the patient's specific situation and surgical risks can we develop personalized treatment plans to achieve the best therapeutic outcomes.
Mount Sinai Heart Center
Professor Gilbert Tang also shared a case of a 94-year-old female with primary mitral regurgitation who experienced recurrent MR after MitraClip™ NT repair and underwent successful re-M-TEER repair. Professor Gilbert Tang emphasized the importance of selecting the patient population for re-M-TEER procedures. To determine the optimal candidates, two key factors must be considered: 1) the mechanism of failure of the previous repair, and 2) the feasibility of redo TEER. Detailed and precise assessment of the mitral valve is required, with comprehensive echocardiographic evaluation recommended. 3D reconstruction is crucial for accurately identifying the mechanism of MR at that moment and planning the redo strategy. Key factors to evaluate include leaflet integrity, length, width, and the risk factors for postoperative mitral valve stenosis.
In this era of vibrant exchange and interaction, the integration of traditional Chinese and Western medicine undoubtedly injects new vitality into the advancement of surgical techniques and the development of the medical profession. Through mutual learning and the exchange of medical concepts and technical methods from different cultural backgrounds, clinicians can continuously enhance their professional competence and skills, providing higher-quality medical services to patients and further advancing healthcare standards. Moreover, such exchanges also contribute to the reform and innovation of medical education, nurturing more medical professionals with international perspectives and innovative spirits.
发表留言
暂无留言
输入您的留言参与专家互动